
11 results
Validation of antibiotic stewardship metrics for genitourinary infection management in Veterans Affairs outpatient settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s35
-
- Article
-
- You have access
- Open access
- Export citation
-
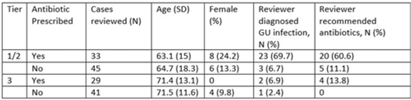
Background: Diagnosis and management of suspected urinary tract infection (UTI) in outpatient settings has been shown to be suboptimal. We previously developed a set of stewardship metrics for UTIs based on electronic health record (EHR) data (Antimicrobial Stewardship & Healthcare Epidemiology 2022;2 suppl 1:S5–S6. doi:10.1017/ash.2022). A tier-based approach was used to more fully capture antibiotic use associated with genitourinary (GU) symptoms and diagnoses. Herein we report a preliminary analysis of validity and reliability of these metrics based on chart abstraction. Methods: The study cohort consisted of patients who visited Veterans Affairs emergency departments or primary care clinics between 2015 and 2022 and who had a GU diagnosis based on International Classification of Disease, Tenth Revision (ICD-10) codes, divided into 3 categories: tier 1 (antibiotics always indicated), tier 2 (antibiotics sometimes indicated), and tier 3 (antibiotics not indicated). Visits related to urological procedures, nontarget settings, or concomitant non-GU infections were excluded. Cases were randomly sampled for manual review from within 8 strata based on tier, use of antibiotics, and visit type. An infectious disease physician and pharmacist abstracted charts using a standardized data-collection instrument. Clinical judgments regarding diagnosis and treatment were recorded on a Likert scale without knowledge of how the patient was managed. The intraclass correlation coefficient (ICC) was used to estimate interrater reliability. Results: To date, 148 cases have been reviewed (50 by both reviewers). Mean (SD) age was 67.5 (15.3) years and 12.2% were female. In a majority of tier 1 and 2 visits in which antibiotics were given, the reviewers found evidence for GU infection (69.7%) and favored prescribing of antibiotics (60.6%) (Table). In contrast, most patients in the tier 3 category who received antibiotics were judged to have noninfectious conditions (eg, benign prostatic hypertrophy) and to not require antibiotics. In the subset of records examined by both reviewers, the interrater reliability of judgments of whether antibiotics were warranted was good (ICC = .704). Conclusions: This preliminary validation provides support for a tier-based approach for stewardship metrics for GU conditions that relies upon electronic data to identify patients for whom antibiotics are generally not indicated.
Disclosures: None

Electronic surveillance criteria for non–ventilator-associated hospital-acquired pneumonia: Assessment of reliability and validity
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 15 March 2023, pp. 1769-1775
- Print publication:
- November 2023
-
- Article
- Export citation
Implementation and outcomes of a clinician-directed intervention to improve antibiotic prescribing for acute respiratory tract infections within the Veterans’ Affairs Healthcare System
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 5 / May 2023
- Published online by Cambridge University Press:
- 15 August 2022, pp. 746-754
- Print publication:
- May 2023
-
- Article
- Export citation
Using machine learning to predict antibiotic resistance to support optimal empiric treatment of urinary tract infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s69
-
- Article
-
- You have access
- Open access
- Export citation
-
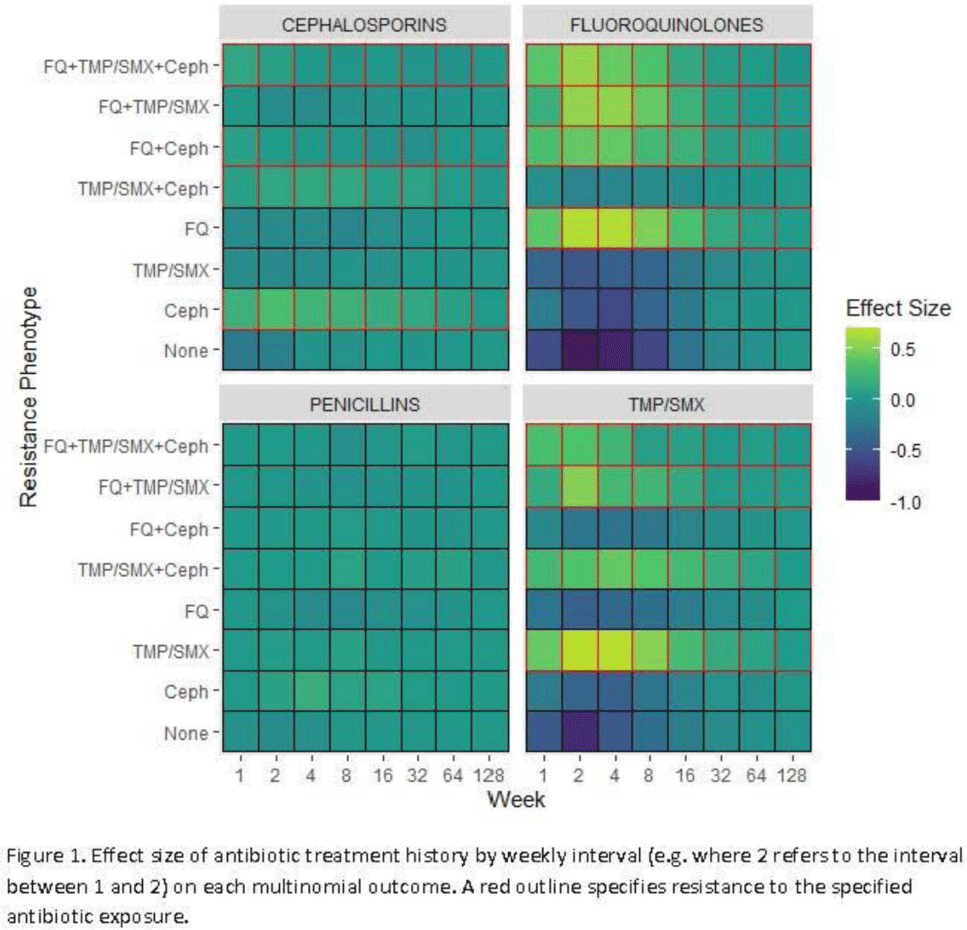
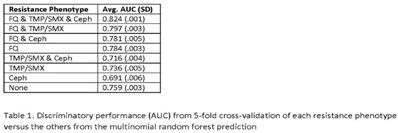
Background: Antibiotic resistance is pervasive in the Veterans’ Affairs (VA) healthcare system, with rates of fluoroquinolone and trimethoprim–sulfamethoxazole (TMP/SMX) resistance approaching 30% in E. coli urinary isolates. The efficacy of antimicrobial treatment is critically dependent on the susceptibility of the infecting pathogen; however, prescription decisions are often made empirically in practice. We analyzed susceptibility profiles of enteric gram-negative rods (Enterobacterales) from clinical urine cultures collected from ambulatory patients receiving care in VA clinics and emergency departments. Our goals were (1) to develop a predictive model to support choice of empiric antibiotics pending results of susceptibility testing and (2) to examine the relationship between past antibiotic exposures and susceptibility profiles to enhance understanding of antibiotic selective pressure. Methods: We obtained 265,076 positive cultures from 157,422 unique patients from 2015 to 2020. We trained random forest multinomial classifiers to estimate the risk of a positive urine culture isolate being resistant to the multinomial outcome: fluoroquinolone, TMP–SMX, cephalosporin, or any combination of these 3 agents. Data sources evaluated for model generation included demographics, comorbidities, trend and seasonal terms, treatment history for multiple antimicrobial treatments summarized using number of prescriptions in weekly intervals, and sample history summarized by number of resistant and susceptible cultures in weekly intervals. Using 5-fold cross validation, we assess the performance of the clinical prediction using the area under the receiver operating characteristic curve (AUC) for each multinomial outcome. In addition to prediction, we modeled the direct effect of treatment on resistance using multinomial group lasso (MGL). This method allows variable selection in variable groupings, such as all variables related to the fluoroquinolone treatment history, which allowed us to assess the effect of a patient’s complete course of treatment on resistance. Results: In cross-validation analysis, our random forest model was best at predicting outcomes with fluoroquinolone resistant phenotypes compared to non–fluoroquinolone-resistant phenotypes (Table 1). From MGL, we found that having a prescription for fluoroquinolone treatment 4–8 weeks prior to a urinalysis was positively associated with fluoroquinolone resistance and negatively associated with fluoroquinolone susceptible phenotypes (Fig. 1). Conclusions: Our results show that a patient’s sample and treatment history are highly predictive of a future resistance. Fluoroquinolone treatment is especially associated with increased risk of fluoroquinolone single- and multidrug resistances. A history of either fluoroquinolone or trimethoprim-sulfamethoxazole (TMP-SMX) treatment is a stronger indicator of a future resistant phenotype than cephalosporin or penicillin.
Funding: None
Disclosures: None


Tier-based antimicrobial stewardship metrics for genitourinary-related antibiotic use in Veterans’ Affairs outpatient settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s5-s6
-
- Article
-
- You have access
- Open access
- Export citation
-
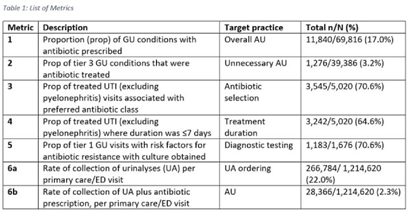
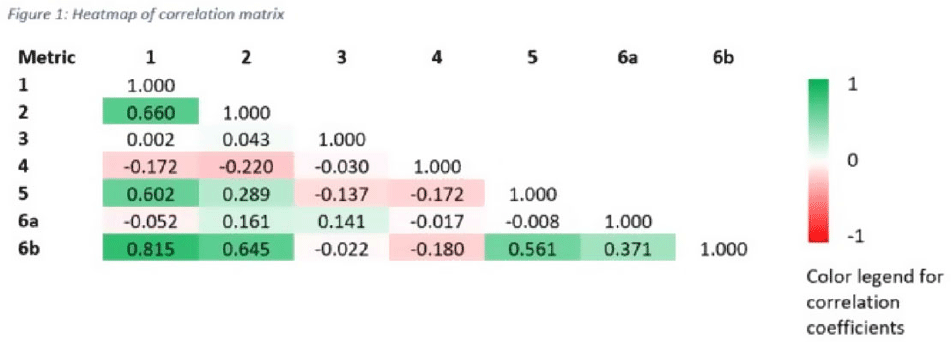
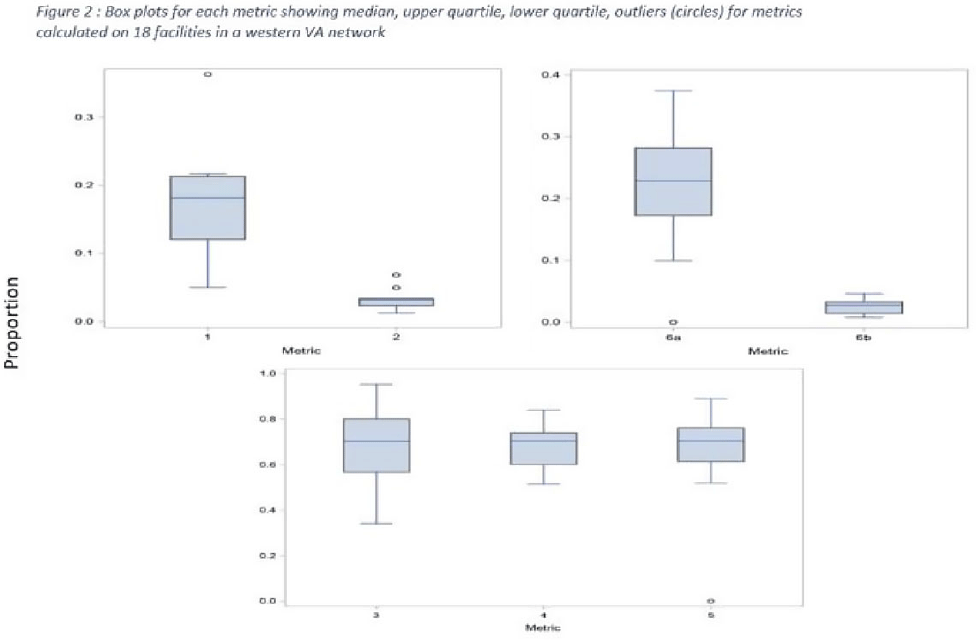
Background: Tracking antibiotic use is a core element of antimicrobial stewardship. We developed a set of metrics based on electronic health record data to support an outpatient stewardship initiative to improve management of urinary tract infections (UTIs) in Veterans’ Affairs (VA) emergency departments (EDs) and primary care clinics. Because UTI diagnostic codes only capture a portion of genitourinary (GU)-related antibiotic use, a tier-based approach was used to evaluate practices. Methods: Metrics were developed to target practices related to antibiotic prescribing and diagnostic testing (Table 1). GU conditions were divided into 3 categories: tier 1, conditions for which antibiotics are usually or always indicated; tier 2, conditions for which antibiotics are sometimes indicated; and tier 3, conditions for which antibiotics are rarely or never indicated (eg, benign prostatic hypertrophy with symptoms). Patients with visits related to urological procedures, nontarget providers, and concomitant non-GU infections were excluded. Descriptive analyses included calculation of the correlation matrix for the 7 metrics and the construction of box plots to display interfacility variability. Results: Metrics were calculated quarterly for 18 VA medical centers, including affiliated clinics, in a western VA network, from July 2018 to June 2020 (Table 1). Tier 3 GU conditions accounted for 1,276 of 11,840 (11%) of GU-related antibiotic use. Metrics 1 and 6b were strongly correlated with each other and were also positively correlated with metrics 2 and 5 (coefficients > 0.5) (Fig. 1). Substantial interfacility variation was observed (Fig. 2). Conclusions: Stewardship metrics for suspected or documented UTIs can identify opportunities for practice improvement. Broadly capturing GU conditions in addition to UTIs may enhance utility for performance feedback. Antibiotic prescribing for tier 3 GU conditions is analogous to unnecessary antibiotic use for acute, uncomplicated bronchitis and upper respiratory tract infections.
Funding: None
Disclosures: None



A Veterans’ Healthcare Administration (VHA) antibiotic stewardship intervention to improve outpatient antibiotic use for acute respiratory infections: A cost-effectiveness analysis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 29 September 2021, pp. 1389-1395
- Print publication:
- October 2022
-
- Article
- Export citation
Increased Return Clinic Visits for Adults with Group A Streptococcal Pharyngitis Treated with a Macrolide
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s295-s296
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Update on Improving Outpatient Antibiotic Use Through Implementation and Evaluation of Core Elements of Outpatient Antibiotic
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s422
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
VA Antibiotic Stewardship Intervention to Improve Outpatient Antibiotic Use for ARIs: A Cost-Effectiveness Analysis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s55
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Development of an Electronic Tool to Measure Daily Appropriateness of Inpatient Antibacterial Use
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s2
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Effectiveness of a multisite personal protective equipment (PPE)–free zone intervention in acute care
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 7 / July 2019
- Published online by Cambridge University Press:
- 07 June 2019, pp. 761-766
- Print publication:
- July 2019
-
- Article
- Export citation
